A Conceptual Clarification and Boundary Framework in Venous Surgery
Dr. Qiang Zhang
Looking forward, the evolution of venous surgery should not be viewed as a conflict between hemodynamic strategies and technological innovation.
Rather, it may be understood as an opportunity to develop techniques that are fully aligned with hemodynamic principles—approaches capable of targeting pathological connections while preserving venous structure and function.
In this perspective, innovation is not defined by the introduction of new devices alone, but by the ability to respect and integrate the physiological logic of the venous system.
The future of CHIVA may therefore lie not in being replaced by technology, but in inspiring technologies that truly embody its principles.
Abstract
The management of chronic venous disease has evolved into two principal paradigms: hemodynamic strategies such as CHIVA and a broad spectrum of endovenous technologies. In recent years, procedures—particularly those based on ablation—have increasingly been described as “CHIVA” or “endovenous CHIVA,” leading to conceptual ambiguity.
This paper introduces the concept of Pseudo-CHIVA to describe interventions that are labeled as CHIVA but do not follow hemodynamic principles. The aim is not to challenge the clinical value of ablative or emerging technologies, but to clarify conceptual boundaries. A framework is proposed emphasizing that CHIVA is defined by strategy rather than instruments, and that the distinction lies in the treatment target, mechanism, and preservation of venous continuity.
Introduction
Chronic venous disease is currently managed through a wide range of therapeutic approaches, from classical surgery to minimally invasive endovenous interventions. Among these, CHIVA (Conservative Hemodynamic Treatment of Venous Insufficiency) represents a distinct paradigm based on correcting pathological hemodynamics while preserving the venous network.
In parallel, endovenous technologies—including radiofrequency, laser, adhesive, and other modalities—have become widely adopted due to their practicality and reproducibility.
However, a convergence of terminology has emerged in clinical communication, where procedures based on venous ablation are increasingly described as “CHIVA.” This overlap necessitates a clear conceptual distinction.
CHIVA as a Hemodynamic Strategy
CHIVA is fundamentally a hemodynamic strategy, not a procedural technique.
Its defining principles include:
- Duplex-guided hemodynamic mapping
- Identification of pathological shunts
- Selective disconnection of reflux pathways
- Preservation of the saphenous trunk whenever feasible
The objective is to reduce venous hypertension by reorganizing flow, rather than eliminating venous structures.
In this context, the saphenous vein is not merely a pathological conduit, but a functional component of the circulatory system, contributing to pressure redistribution and long-term adaptation.
Ablation and Technological Approaches
Endovenous ablation techniques, including radiofrequency and laser, have demonstrated clinical effectiveness and are widely used in contemporary practice.
These techniques are based on a different therapeutic logic:
Ablation eliminates reflux by closing or destroying a venous segment
CHIVA corrects reflux by modifying flow while preserving venous continuity
These approaches are therefore distinct, though not mutually exclusive in clinical value.
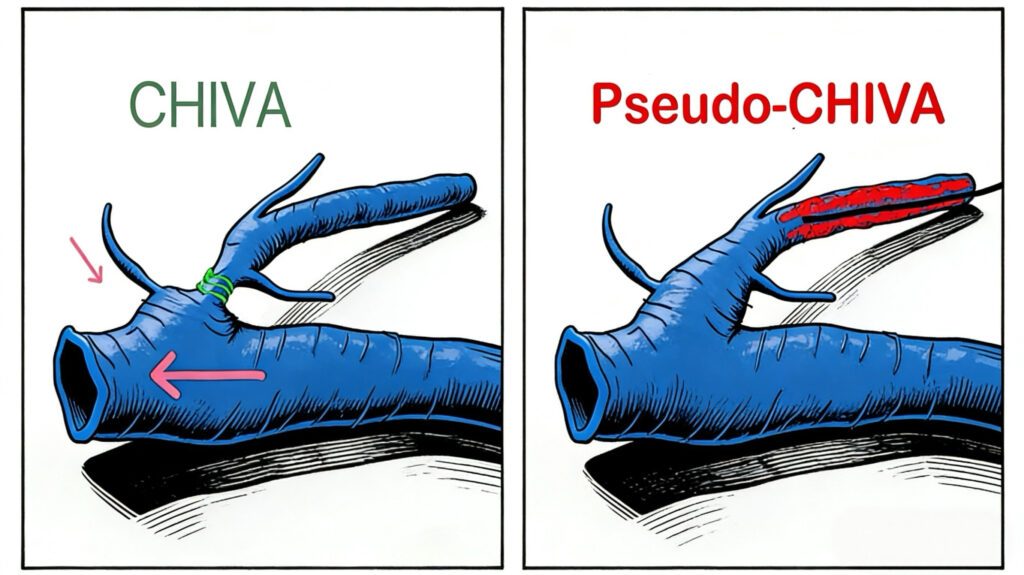
Definition of Pseudo-CHIVA
To address conceptual ambiguity, we propose: Pseudo-CHIVA
Definition:
Pseudo-CHIVA refers to interventions that are described or presented as CHIVA but do not follow hemodynamic principles of flow preservation, and instead rely on venous segment destruction or non-hemodynamic strategies.
Pseudo-CHIVA is therefore defined not by technology, but by: misalignment between terminology and hemodynamic mechanism.
Boundary Framework: Target, Mechanism, and Continuity
The distinction between CHIVA and non-CHIVA interventions is not determined by:
- Device type
- Degree of invasiveness
- Length of treatment
It is defined by three fundamental dimensions:
1. Target
CHIVA: pathological shunts (connections)
Non-CHIVA: venous segments
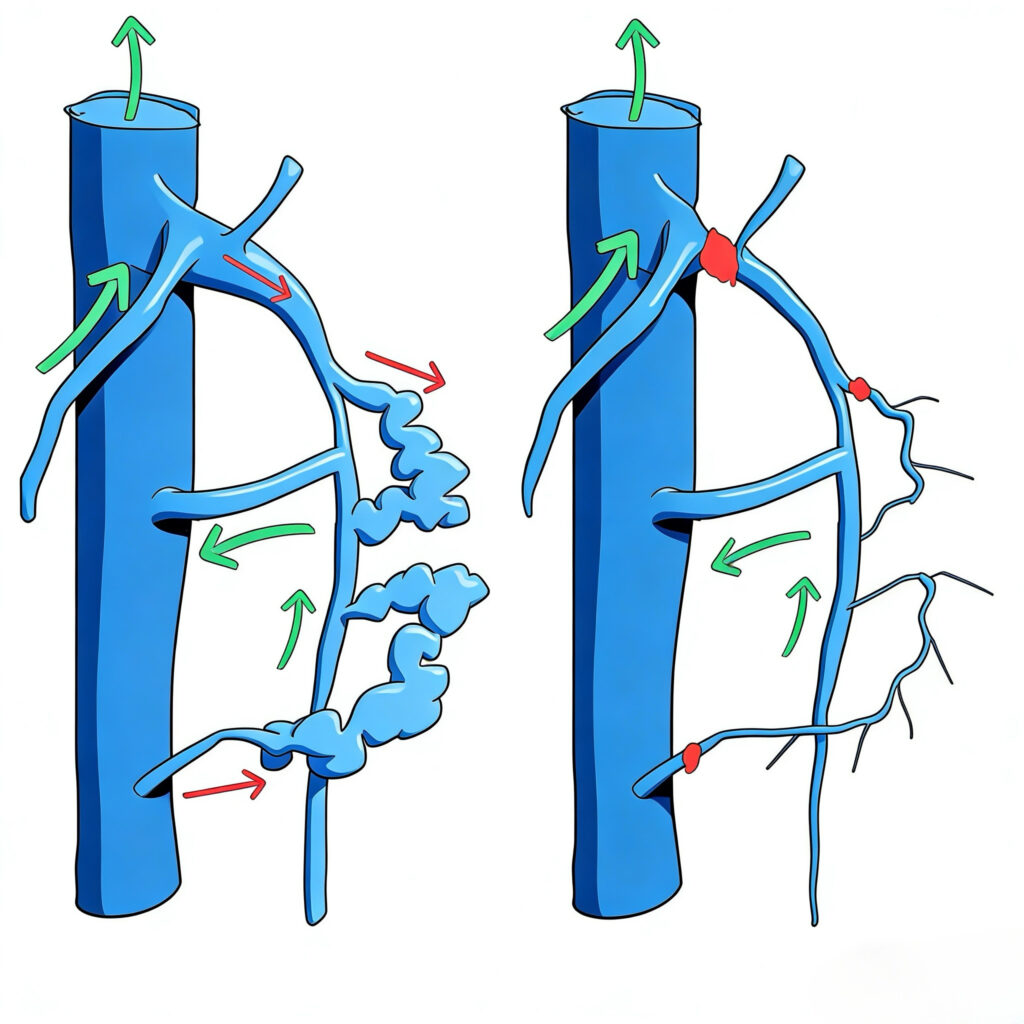
2. Mechanism
CHIVA: disconnection and flow redistribution
Ablation: destruction and flow elimination
3. Continuity
CHIVA: preservation of saphenous trunk continuity
Ablation: segmental interruption
CHIVA treats connections, not segments.
Junction-Level Limitation of Ablation
A key hemodynamic issue lies at the saphenofemoral junction (SFJ), where reflux commonly originates.
In current endovenous practice, ablation requires maintaining a safety distance (typically 1–2 cm) from the SFJ to avoid deep vein complications. Consequently:
👉 ablation cannot directly target the pathological junction
Instead, it treats a downstream venous segment.
This has important implications:
The pathological connection is not directly disconnected
A segment of the conduit is eliminated instead
Ablation cannot treat the junction — it can only bypass it by removing the conduit below.
Thus, even when technically precise, ablation does not constitute connection-specific hemodynamic correction.
Short-Segment Ablation vs Hemodynamic Disconnection
Short-segment ablation (e.g., 5–10 cm) is sometimes presented as a more targeted approach. However, the distinction is not determined by length.
Although both ligation and short-segment ablation may result in permanent occlusion, they are not conceptually equivalent.
- Hemodynamically guided ligation aims to disconnect a pathological shunt
- Ablation destroys a venous segment itself
The distinction therefore lies not in reversibility or extent, but in:
- target (connection vs segment)
- mechanism (disconnection vs destruction)
- impact on trunk continuity
Even a short ablation remains a form of segmental destruction. The difference lies not in length, but in principle.
CHIVA-Compatible Approaches
It is important to emphasize that not all non-traditional or minimally invasive techniques fall outside the CHIVA framework.
Certain interventions may be CHIVA-compatible when they:
- Are guided by hemodynamic mapping
- Target pathological connections
- Preserve trunk continuity
- Aim to modify flow rather than eliminate it
This reinforces that the distinction is conceptual rather than technological.
Why Terminology Matters
Accurate terminology is essential for:
- Clinical education
- Scientific communication
- Interpretation of outcomes
- Patient understanding and informed consent
When fundamentally different treatment strategies are described using the same term, conceptual clarity is compromised.
The introduction of Pseudo-CHIVA aims to restore this clarity.
Conclusion
CHIVA and endovenous ablation represent two fundamentally different approaches to the management of chronic venous disease.
The distinction lies not in technique, but in:
- therapeutic target
- underlying mechanism
- preservation of venous function
The concept of Pseudo-CHIVA provides a framework to describe situations in which these distinctions are blurred.
Its purpose is not to oppose technological innovation, but to ensure that: medical terminology accurately reflects hemodynamic reality.
The future of venous surgery lies in the synergy between advanced technology and hemodynamic intelligence. We look forward to an era where innovation does not merely simplify the destruction of a vein, but empowers the physician to restore physiological balance with surgical precision.